



Statins: Akira Endo’s Revolutionary Contribution to Medicine
And some Controversy

In today’s Substack:
All about statins
What they are
How they work
Are they truly effective: the controversy
All about Akira Endo
I am writing today’s Sub stack in honour of Akira Endo, a Japanese Biochemistry scientist who unfortunately passed away on the 5th of June. He is the reason why Statins, or cholesterol lowering drugs, exist on the planet and why so many individuals are protected from heart disease and stroke.
But first….
What are statins?
Statins are a type of medicine that is used to lower the blood cholesterol. Some of you may have heard of Atorvastatin, Rosuvastatin, or even Pravastatin. They are usually taken once a day, at night, and are given to those who have high cholesterol based on a blood test. They can also be given to those who are at a high risk of heart attack or stroke.
For an explanation on why one would need to lower their blood cholesterol to decrease risk of heart disease or stroke, read one of my previous articles 😉

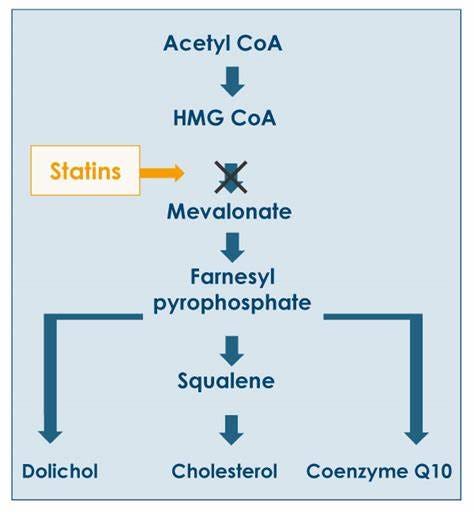
How do they work?
The aim of a statin is to lower the cholesterol in the body. It mainly works on total cholesterol, and LDL cholesterol.
The drug targets enzymes in the liver that are responsible for synthesising the base molecule for cholesterol. This enzyme is known as HMG-Co-enzyme A- Reductase (don’t ask me why).
The statin likes to sit on the enzyme and occupy all its binding sites, so that there are none left to make cholesterol! However, once the drug is metabolised and excreted by the body, one must take the tablet again. That’s why it’s a once- a- day tablet, sometimes taken life-long.
What are they used for?
Naturally, they are used in conditions wherein the cholesterol content of the blood is too high. So, those who suffer from…
- familial hypercholesterolemia
- have had a heart attack, or stroke, and need secondary prevention.
- are at a high risk of heart disease and need primary prevention.
…all need this medicine.
Do they really work?
If you have heard of a statin, you have heard of the controversy surrounding it: Are they really useful?
Secondary prevention is when a therapy is used after the disease or condition to decrease the risk of it happening again- like giving statins after a heart attack. In this case, the medicine is given to “non-healthy” individuals.
What about healthy individuals? Is it justified to give a statin therapy to someone who is healthy otherwise, and has never had a heart attack or stroke before?
This is where I started to get lost. As I write these words, my head is swimming with published articles arguing for one side, or the other.
The Framingham heart study was one of the first large trials to assess cardiovascular disease and its risk factors. It is famous for identifying smoking as a significant risk factor and has helped us identify important therapies like Aspirin. Its an extremely fascinating study and I might write about it one day! The study has not concluded yet, despite beginning in 1948, and is now studying its third generation of participants.
The Framingham heart study identified LDL cholesterol as a risk for cardiovascular disease. Multiple studies after that were designed to confirm the association.
Those who suffer from cardiovascular disease also have high LDL cholesterol
However, there are other researchers who argue that association does not always mean causation.
Dr. Robert DuBroff MD is a Cardiologist most famous for challenging the Cholesterol hypothesis (CH). His paper titled “Cholesterol confusion and statin controversy” challenged the research trials supporting statin therapy by stating that their benefits may have been overstated.
An excerpt from this paper is as follows:
“Early statin trials reported significant mortality benefits, yet serious concerns have been raised in some studies regarding biased results, premature trial terminations, under reporting of adverse events, high numbers of patients lost to follow-up and oversight by the pharmaceutical company sponsor. Heightened awareness within the scientific community regarding problems in clinical trial conduct and analysis - exemplified by the unreported risk of heart attacks in patients taking the pain killers Vioxx and Celebrex - led to new regulatory rules for clinical trials in 2005. Curiously, statin trials conducted after 2005 have failed to demonstrate a consistent mortality benefit.”
Additionally, statins have side effects that can significantly lower the quality of life. Those who consume high dose statins might frequently complain of muscular and body aches. They also must keep a close watch on their liver and perform tests regularly to ensure no serious adverse effects have occurred. In this case, is it justified to start someone on a statin based purely on a calculation of risk (primary prevention)?
Quite frankly, I don’t know what the answer is. I have now worked in a cardiac and stroke unit for 3 months and see heart attack and stroke patients daily. Here, we measure the level of cholesterol first by doing a blood test. We then decide on the strength or dose of a statin that the patient needs based on how bad their cholesterol is. This makes complete sense to me, but I am not a cardiologist and cannot claim to know any better! (haha). I also agree with Dr. DuBroff’s main opinion that “nothing can replace Lifestyle therapy”. Smoking cessation, dietary adjustments, and a significant amount of exercise will help the patient far more. The problem is that patient uptake of this therapy is far less. It’s harder to convince a patient to stop smoking, and much easier to prescribe a pill!
The history of statins: Akira Endo’s work
Akira Endo was born in Japan into a farming family in 1933. After completing his training in Agriculture at the Tohoku University, he worked for the Sankyo pharmaceutical company in Tokyo. While here, he began a project than spanned two years. His aim was to identify a cholesterol biosynthesis inhibitor. He wanted to find something that would stop the synthesis of cholesterol in a mammal body.
As most experiments are, this one was done on rats. Rat liver membranes were extracted and used as the medium in which cholesterol is synthesised. These membranes converted radioactive acetate into cholesterol. He then exposed this experimental set-up to 6000 different fungal extracts to see which extract would inhibit the synthesis of cholesterol.
If the text is getting too chunky, ignore the last paragraph and think of it like this: He created an experiment that wanted to look for a fungus that would stop the synthesis of cholesterol. He used a rat’s liver as the cooker of cholesterol and knew that it would be a fungus that would stop the rat liver from cooking. So, one by one, he went through 6000 different fungi and put them on the liver and checked to see if cholesterol would be made. He was able to find two fungal extracts that did the job!
These fungal extracts were the pre-cursors of the modern-day statins we see today.
Akira Endo talking about his work
Cool, isn’t it?
Note- this article talks about controversy in medical therapy. This is an unavoidable circumstance, as the world of medicine is constantly changing. Controversy is good, because at the end of the argument, what is best for the patient and the population will always rise!
Happy reading 😊