



Mpox: The next pandemic?
This is all you need to read.

Viruses are real buggers. They can create extreme havoc (like we saw in 2020) and don’t die easily. Since the pandemic, the world seems to be on high alert for strange viruses that simultaneously affect a large group of people. One such virus is the Mpox virus. Is this the next COVID-19?
The short answer to that question is- we don’t know, yet. However, the disease has created enough alarm to ring the bells of the WHO and initiate global action. Here’s why-
In 1958, a small group of monkeys were shipped from Singapore to Denmark. These monkeys were innocent banana-eating creatures, but the human population seemed to take a special interest in them when one of their clan fell sick. The group of monkeys had a disease that looked. A lot like smallpox, but was not quite it.
After studying the diseased monkeys in great detail, it was discovered that those monkeys were infected by a virus with the same genetic makeup as smallpox. However, presented differently, thus they named the virus monkeypox.
There are loads of viruses and other organisms that affect animals, and we never really hear about it. In fact, the first case of monkeypox in a human was described in a 9-month-old baby in the democratic republic of Congo over 10 years after it was initially discovered. So, why all the fuss now?
Recently, the cases of mpox have risen dramatically. The main focus of the infection seems to be in the Democratic Republic of Congo (DRC) where the mpox infection is not an unknown fact.
Then, out of seemingly nowhere, a large outbreak of mpox cases occurred that initially began in Nigeria and then spread globally. Over 100,000 people were affected, and a large number died.
Just as suddenly as it came, the outbreak died down and the general public stopped thinking about it.
However, on the 14th of August, the WHO declared a global health emergency over a rise in the number of mpox cases. By declaring this, it means to stimulate efforts to contain the disease as it is something that was serious and sudden, has implications crossing state boundaries, and requires a large international effort. Just a day later, a single European case was reported. The international community really seemed to wake-up at that point.
But first, what is MPox?
Mpox stands for Monkeypox. It is a virus very similar to the smallpox virus. Smallpox was a condition that caused a lot of trouble back in the day, but in the early 1980s, the WHO declared that we had eradicated the condition and removed the smallpox vaccination program.
Officials acknowledged that the vaccination for smallpox was probably providing some amount of protection against monkeypox, but decided that the issue at the time was very small, and that there weren’t enough cases to cause alarm.
This virus leads to symptoms of a fever and flu-like illness (AKA the prodrome) and later leads to painful blisters over the face, hands, and even the feet and soles. Most cases, however, seem to present with genital lesions.
Some of the initial cases that presented in Nigeria came with genital lesions. As cases began to increase, the history of “sexual contact” seemed extremely common. Men who have sex with men, or those who visited sexual workers seemed to be amongst the highest proportion infected.
Others didn’t have this story, like young children, so it became clear that close contact is the mode of spread, sexual or otherwise.
As with any viral illness, there isn’t really a treatment. I like bacteria because we can, in most cases, zap them with antibiotics. Unfortunately, we don’t have a lot of antivirals lying around, and the only way to treat a viral infection is with time, and our bodies’ efforts.
We do have vaccines, however. The two vaccines currently in use for mpox are recommended by WHO’s Strategic Advisory Group of Experts on Immunization.
It already sounds like we are a lot more prepared this time round than we were for COVID-19…
The Strain conversation
Right, let’s go deeper into the microbiology of mpox, shall we?
Mpox is a double-stranded DNA virus and looks a bit like this:
A clade of viruses is a group of viruses that have a single ancestor. It is a phylogenetic definition and can be simply thought of as a group of siblings that have come from the same mother.
Since its discovery, the mpox has been studied and its tree of descendents mapped out.
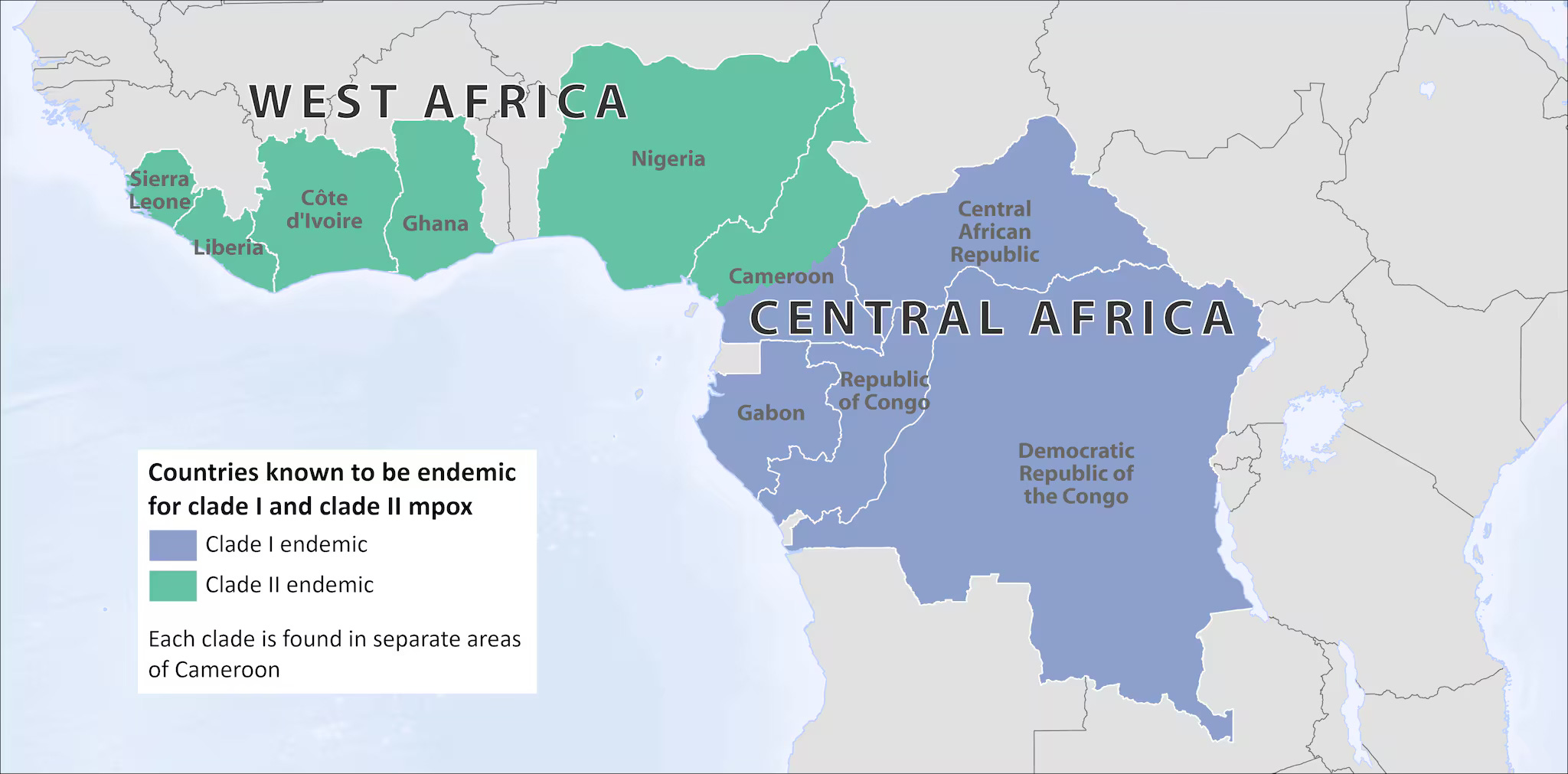
We traditionally know of two clades of the mpox.
One, a more dangerous one, that can cause a high degree of mortality is known as the Congo Basin, Central African or Clade I
The second is less virulent and is known as the West African clade or Clade II.
The two clades are different in their genetic makeup. The difference in the genetic sequence is in important parts that determine how damgerous the virus can be, thus explaining why Clade I is more dangerous than Clade II. These clades are further split into Ia, Ib, Ida, and IIb based on the sample principle.
The global outbreak in 2022 was caused by the Clade IIb mpox virus. This time around, however, we think its Clade Ib.
The DRC has, as I mentioned earlier, had been brewing cases of mpox. Clade Ib mpox was isolated in the DRC last year in November, but the alarm occurred when it was isolated outside of the country for the first time. The case isolated in Sweden was confirmed as Clade Ib MPXV. I read somewhere that the Clade Ia tends to cause infection in children whereas Clade Ib tends to infect adults, but I could not find a reference for it (although it does make sense).
Transmission
As of now, we know 2 routes of transmission:
Skin-to-skin contact- If you touch the rash of someone who has mpox, the virus will start to replicate in your skin cells, and then spread to your lymph nodes. From there, it may spread to the rest of the body.
Respiratory secretions: Usually only comes from someone who is heavily infected with mpox. When a patient coughs, they may send out infected respiratory droplets. These settle onto an unaffected person’s mouth and nose and may lead to an infection. A long face-to-face contact period is required for this.
Fomites: From the bedding, clothing, or other items of an mpox patient
Vertical transmission: From mother to unborn child.
What to watch out for
Once exposed to mpox, it can take from 5 days up to 3 weeks to begin displaying symptoms. Patients usually suffer from a fever, weakness, a headache and other general flu-like symptoms. Their lymph nodes may swell up as well.
From 1 day to 5 days after the fever appears, a rash may develop that begins on the face or genital area and may spread to other parts of the body. I won’t describe the rash here as it doesn’t sound very nice, and we don’t need the stigma. Essentially, it’s an uncomfortable not-so-nice-looking rash that eventually scabs off.
Conclusion
As usual, there is still a lot that we don’t know. Many questions surrounding the origins of this strain and how best to tackle it abound in the scientific domain, but it’s important to focus on what we do know.
The mpox disease is something worth looking out for.
We now know its symptoms and transmission.
We know there is a vaccine and it has been around for a while.
Please fact-check everything you read!
As always,
Happy reading!